
June 9, 2025 | Jeanna Vazquez
Nationally Recognized for Sustainability in Health CareJacobs Medical Center and Hillcrest Medical Center at UC San Diego Health have been named Top 25 hospitals in the nation for exceptional sustainability efforts.

June 9, 2025 | Jeanna Vazquez
Nationally Recognized for Sustainability in Health CareJacobs Medical Center and Hillcrest Medical Center at UC San Diego Health have been named Top 25 hospitals in the nation for exceptional sustainability efforts.

June 3, 2025 | Annie Pierce
Psychiatry Residency Program to Launch in Imperial CountyUC San Diego Health and Imperial County Behavioral Health Services launch region’s first psychiatry residency program in Imperial Valley.
May 20, 2025 | Kim Coutts
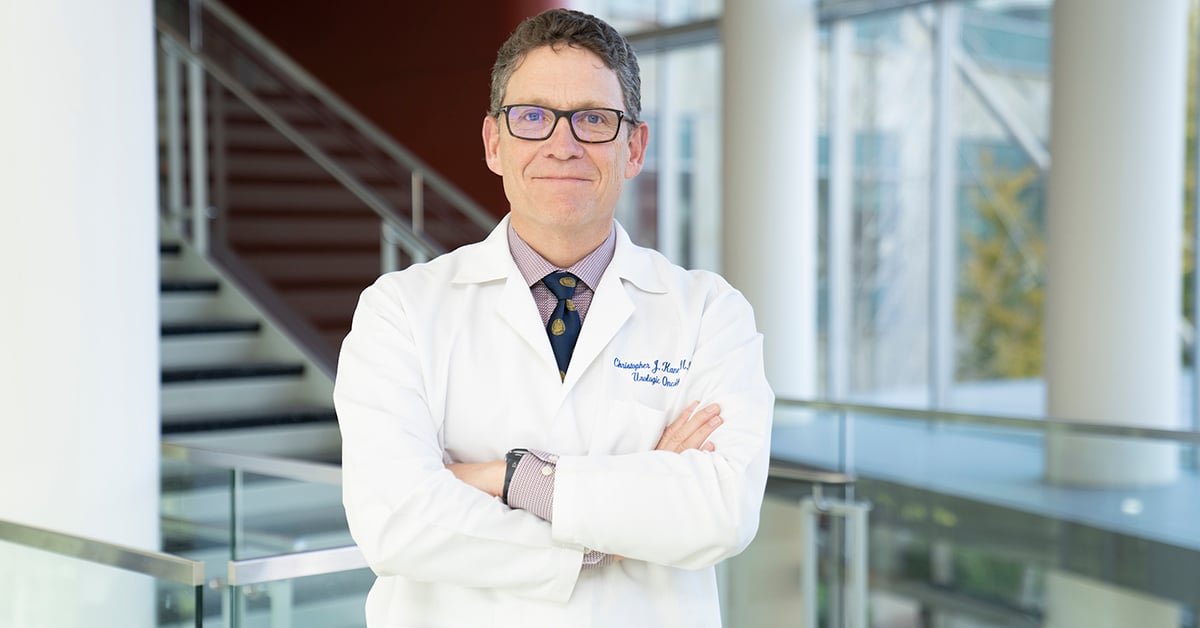
Christopher Kane Appointed President of American Board of UrologyChristopher Kane, MD, CEO, UC San Diego Health Physician Group, appointed president of American Board of Urology.

At just 13, Lexi Rains faced hearing loss from a rare brain tumor. Discover how expert surgeons at UC San Diego Health preserved her hearing and changed her life.

Not all symptoms are harmless. Learn about 10 warning signs — like chest pain, sudden confusion and unexplained weight loss — that could signal serious or life-threatening health issues.

NIH funding cuts could threaten U.S. medical research. A top neurosurgeon warns of risks to innovation and patient care.

The community comes together to learn more about the benefits of clinical trials during an event held at Moores Center Center at UC San Diego Health.
Not all symptoms are harmless. Learn about 10 warning signs — like chest pain, sudden confusion and unexplained weight loss — that could signal serious or life-threatening health issues.

The same-day cancer care clinic at UC San Diego Health provides fast, expert treatment for urgent cancer-related symptoms, improving patient care and quality of life.

Acetaminophen is in more than 600 medications and is the top cause of liver injury in the U.S. Learn how to use it safely and avoid accidental overdose.

Alison Moore, MD, MPH, has been named president-elect of the American Geriatrics Society. In this Q&A, she offers insight into her field of geriatrics medicine.
Not all symptoms are harmless. Learn about 10 warning signs — like chest pain, sudden confusion and unexplained weight loss — that could signal serious or life-threatening health issues.
The community comes together to learn more about the benefits of clinical trials during an event held at Moores Center Center at UC San Diego Health.
At just 13, Lexi Rains faced hearing loss from a rare brain tumor. Discover how expert surgeons at UC San Diego Health preserved her hearing and changed her life.
Patient Katharine Unetic shares her success story with TMS therapy, a non-invasive, FDA-approved intervention for treatment-resistant depression.